Nearly one in ten hospitalized patients will get a urinary catheter. This procedure, generally used for emptying the bladder when it cannot do so naturally, has severalindications. Practiced since antiquity, there are various forms of bladder catheterization today, including indwelling, evacuation, and even self-catheterization.
Things to know
The bladder is emptied by inserting a sterile catheter into the urethra through the urinary meatus.This procedure falls within the prescribed role of the nurse (French Public Health Code Art. R4311-7), although the initial catheterization in men with urinary retention must be performed by a doctor (PHC Art. R4311-10).
The bladder emptying problem can result from:
- a subvesical blockage (most frequent)
- a change in neurologic signaling
- more rarely, defective bladder contraction.
In addition to drainage, a catheter can also be used for taking alabspecimen, administering medication, or irrigation.
We must also be aware of the contraindications to bladder catheterization, which include urethral stricture and trauma to the urethra, especially in cases of multiple trauma (pelvic fracture) or acute prostatitis.
There are several types of catheters:
- Indwelling: Continuous emptying of the bladder, intended to remain in place.
- Evacuation: One-time emptying of the bladder, does not stay in place.
- Intermittent: Identical to the evacuation catheter, this is repeated several times a day.
- Self-catheterization: Catheterthat is inserted by the patient, part of the intermittent catheterization process.
Selection of medical devices.
This procedure requires a good knowledge of the equipment, which will differ by patient and indication. The catheter may have:
- 1 lumen: No balloon. To drain urine only. Indicated for evacuation catheterization, this may be straight or curved (coudé). it isalso used to administer medication to the bladder (e.g. in chemotherapy).
- 2 lumens: One to drain urine and the other to inflate the balloon that holds it in place. The Foley® catheter in latex for short-term(< 8 days), or silicone for long-term (> 8 days). This can be fitted with a temperaturesensor if the indication requires it.
- 3 lumens: The third lumen is used for irrigation in cases where there is a risk of clotting due to hemorrhage. This requires the use of a Hematuria catheter (or Couvelaire), ora two-way catheter if irrigation is continuous.
The diameter of the catheter is determined based on the patient’s age, sex and body size.
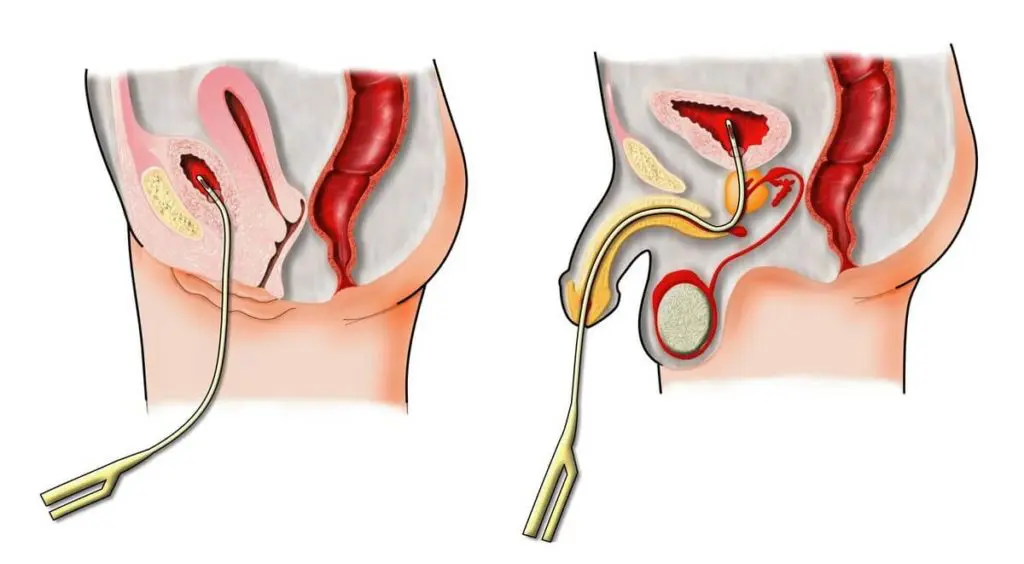
Urinary catheterization is different in men and women due to their different anatomy. In men, the presence of the prostate and the length of the urethra (about 15 cm compared to 3.5 cm in women) will increase the risk of trauma. The risk of a urinary tract infection, however, is greater in women, where the urinary meatus leads to the vulva between the clitoris and the vaginal opening.
More than just technique
The catheterization technique is a source of apprehension for both student nurses and young nurses, yet it calls on much broader expertise. Because this procedure involves patients’ “privates,” interpersonal skills are key, especially when performed on an alert patient, or even when the patient discovers the catheter after surgery.
Getting the patient to accept both the procedure and the device is an integral part of care.
In indications for intermittent catheterization, particularly in spinal cord injuries, the procedure also requires therapeutic education skills.It is the nurse who teaches patients how to insert their own catheters. An intake interview will determine the patient’s pathology, cognitive resources, social environment, functional abilities, stress level and motivation.
This is followed by education on anatomy and hygiene, andfinally assistancein choosing the equipment, especially the catheter: size, length, curved or straight, pre-lubricated (hydrophilic) or needing lubricant (non-hydrophilic).
The patient is always encouraged to self-catheterize, but this requires functional and cognitive abilities as well as appropriate therapeutic education. This practice has a dualbenefit: reducing the incidence of urinary tract infections and improving the patient’s quality of life by not requiring them to have an indwelling catheter.
From papyrus to procedure
The first traces of urinary catheterization are found in 3000 BCE, in a description on an Egyptian papyrus. The use of a bronze S-shaped catheter, adapted to the age and sex of the patient, was common in Greece in 400 BCE.
The devices have changed over the centuries as the risks became known, particularly the risk of infection. The biggest change is in the materials: reed, straw or even gold or silver catheters have been usedin the past. The first rubber catheters appeared in the 18th century. Unfortunately the rubber in that era was brittle and left particles in the bladder. The quality of catheters improved towards the end of the 19th century, but latex catheters did not appear until 1930. That was the year the American urologist Dr. Frederic Foley invented the balloon catheter.
The concept of intermittent catheterization was introduced during WWII, with the large number of spinal cord injuries and particularly due to the risk of infection, which at the time was called “catheter fever.”
Preventing infection remains at the heart of catheter care today. In fact, 30% of nosocomial infections are urinary tract infections, and three-quarters of these are associated with catheter use. This is why procedures are in place. It is essential that caregivers follow the recommendations of the CLIN (French Committee to Combat Nosocomial Infections) and the SF2H 2015 (French Society for Hospital Hygiene).
